
In 2016-2017, 606 New Zealanders took their own lives. This is the highest rate since statistics started to be collected in 2007. It is likely to be under-reported, as there deaths where suicidality is difficult to ascertain. This is a shocking loss for the whānau of those people, for their community, for all of us. There are myriad reasons that lead people to take their own lives, both personal and societal. It is the latter that I am writing about here, but that is not to downplay the former.
[If you are feeling suicidal, please talk to someone right now. There is also a list of services that can help you at the end of this blog.]
Our Aotearoa New Zealand society is sick. We are promoting dominant cultural values and goals that are causing the death of people in our society:
- the importance of celebrity;
- the perfection of the physical form (a war against fat);
- emotional denial and disconnectedness (the harden up culture);
- a fear of others;
- our youth as a threat (youth as the risk);
- a society in service of an economy (the worship of productivity, growth and profit);
- the sin of sadness and pain (happiness is correct, suffering is wrong).
All of these and potentially other values communicate that the right and correct life is the very life that is unattainable to most of our society. For young people, in the midst of their formation, it is more than unattainable; it is a death cult. These dominant cultural values and goals are a form of illness that results in people being trapped in unhappy and unfulfilled lives.
That we might be unhappy in a society that presents the unattainable as the desirable is not a new thought. The 19th century French pioneer sociologist Emile Durkheim borrowed the word ‘anomie’ (said: AN-oh-me) from French philosopher Jean-Marie Guyau to describe this state. Characterised by an absence or diminution of standards or values (referred to as normlessness), and an associated feeling of alienation and purposelessness, Durkheim believed that anomie is common when there is a significant discrepancy between the values commonly professed and what was actually achievable in everyday life. In Durkheim’s view the division of labour that had been prevalent in economic life since the Industrial Revolution led individuals to pursue egoistic ends rather than seeking the good of a larger community.
Robert King Merton also adopted the idea of anomie to develop Strain Theory, defining it as the discrepancy between common social goals and the legitimate means to attain those goals. Merton’s theory focuses upon various acts of deviance, which may be understood to lead to criminal behaviour. It differs somewhat from Durkheim’s in that Merton argued that the real problem is not created by a sudden social change, as Durkheim proposed, but rather by a social structure that holds out the same goals to all its members without giving them equal means to achieve them. It is this lack of integration between what the culture calls for and what the structure permits that causes deviant behaviour. Deviance then is a symptom of the social structure. Simply put, in a market liberal democratic capitalist society like Aotearoa New Zealand, overemphasis on material success and lack of opportunity for such material success leads to crime.
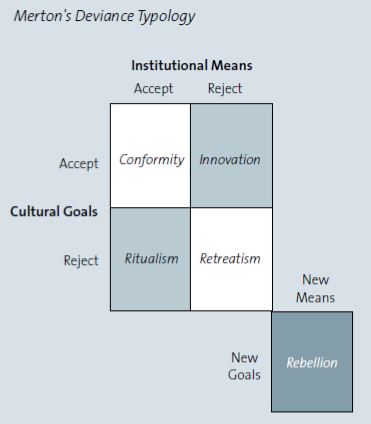
‘Strain’ is caused by the restricted access to culturally approved goals and means. Merton presents five modes of adapting to strain:
- Conformity: Merton recognises conformity as the most common type of the five modes. Individuals accept both the cultural goals as well as the prescribed institutional means for achieving those goals. Conformists will accept, though not always achieve, the cultural goals of a society and the means approved for achieving them.
- Innovation: Merton identifies a change in the perspective of those people who have shifted to innovation. They accept cultural goals but have few legitimate means to achieve those goals. Thus they innovate (design) their own means to get ahead. The means to get ahead may be regarded within a society as criminal acts (though not always regarded as such by the individuals or social group themselves).
- Ritualism: Another adaptation is for individuals to abandon the cultural goals they once believed to be within their reach and dedicate themselves to their current lifestyle. They play by their own or group’s rules and norms, and have a self-perceived safe daily routine. Many members of an urban lower socio-economic population and/or disadvantaged minorities will experience slightly increased, self-perceived success, but this is ultimately short-lived and undervalued within the dominant society.
- Retreatism: Identified by Merton as the escapist response, retreatism occurs when people become practical dropouts of society (as seen against cultural goals and norms). They give up all goals and efforts to achieve success because they view it as an impractical, impossible, almost imaginary and irrational possibility. Retreatism is the adaptation of those who give up not only the cultural goals but also the institutional means. Their inability in obtaining success by legitimate means excludes them from society, often resulting in retreat into substance abuse, housing insecurity, health deprivation and criminal activity. They escape into a non-productive, non-striving lifestyle.
- Rebellion: Merton suggests that by the time people reach the mode of rebellion, they have completely rejected the story that everybody in society can achieve success and have loomed into a rebellious state. They neither trust the valued cultural goals nor the legitimate institutional means. Instead, these people create their own goals and their own means, by protest or revolutionary activity. Unlike the other modes of response, rebellion is a group response, seeking to replace the cultural goals and/or the institutional means of an unequal social system.
Structuralist models like Merton’s are problematic, not least because they try and describe the complexity of life in a pre-conceived box. Nevertheless, as an exercise in reflection, Strain Theory provides some insight.
The troubling concept of retreatism is a part of the malaise we see in our communities and in our world leading rates of drug and alcohol abuse. This often exacerbates, or is exacerbated by, mental illness, and is again apparent in our high suicide rates. What’s worse is that these abuses and health concerns are regarded as normative: for those they touch, it is just a part of our community; for those whose wealth immunises them from the worst impacts, it is what they expect from poverty. Our education and health systems are of little assistance as they focus on moving us towards ‘conformity,’ that middle ground of experience we think we can measure. This is not to insinuate that everyone who is denied easy access to society’s baubles became deviant, rather that the response, or modes of adaptation, depend on the individual’s attitudes toward cultural goals and the institutional means to attain them.
The systemic issue is we have no language or leadership to discuss our values and our goals as a society. So for most of our problems of inequality (and suicide in a societal and communal sense is derived from an increasingly inequal society) our response, our programmes, our services are essentially individualist: so people can easily blame themselves for their lack of achievement. In doing so, they implicitly help society preserve and maintain itself. Despite our society’s manifest social inequalities, people blame their own shortcomings – and fail to call into question the system’s inadequacies.
A major inadequacy of the system concerns the overwhelming intensity of the message that more is good, that more material possession and more consumption is at the heart of what it is to be happy. This message is internalised at some level by all individuals and the argument that somehow meaning can be derived from this is one of the great illusions of modern life. This belief creates an intense fear of failure and an inability to conceive of enough.
British psychologist Oliver James asserts the more unequal a society, the greater the unhappiness of its citizens. James also believes that higher rates of mental disorders are the consequence of excessive wealth-seeking in consumer societies. World Health Organization data shows that English-speaking nations have twice as much mental illness as mainland Europe. James explains this discrepancy as the result of ‘Selfish Capitalism,’ the neo-conservative or market liberal political governance found in English-speaking nations as compared to the less selfish capitalism pursued in mainland Europe.
Any approach to suicide that attempts to work with individuals and their whānau but is silent on the inequalities in our society will not slow the regular, tragic flow of deaths. We need a rebellion against the destructive values and goals at the rotten heart of our system. There are little lights of hope; many schools and kura teach, speak and model alternative values every day, encouraging their children and young people to see life differently. The challenge is that there is no change until the word is made flesh; that miracle is wrought by leadership of clarity and integrity at all levels, from your home to the halls of Parliament.
Lifeline: 0800 543 354 – Provides 24 hour telephone counselling
Youthline: 0800 376 633 or free text 234 – Provides 24 hour telephone and text counselling services for young people
Samaritans: 0800 726 666 – Provides 24 hour telephone counselling.
Tautoko: 0508 828 865 – provides support, information and resources to people at risk of suicide, and their family, whānau and friends.
Whatsup: 0800 942 8787 (noon to 11pm)
Kidsline: 0800 543 754 (4pm – 6pm weekdays)
The Lowdown: thelowdown.co.nz – website for young people ages 12 to 19.
National Depression Initiative – depression.org.nz (for adults), 0800 111 757 – 24 hour service
If it is an emergency or you feel you or someone you know is at risk, please call 111
For information about suicide prevention, see www.mentalhealth.org.nz/suicideprevention.

Great piece Graham.
Only comment and its trival. For some people pronunciation of the word anomie is an issue. Maybe add a “how to pronounce”. SF
>
Your wish is my command.
Such a thoughtful piece – your summary of the kind of values that this society currently ‘rates’ was on point. Thank you
Kia ora ki a koe.
Tena koe Graham, thank you for the wonderful thought provoking korero. You are so right. The stats are scarey! I’m wondering if you can post to Facebook please so that I can share to wider hapu whanau and friends.
I really enjoy reading your blog. You articulate so well what I’m sure many of us are feeling
Nga mihi
Kia ora Ripeka, thank you. It is on Facebook (though you can also do it using the buttons at the bottom of the blog) on my account. It’s Public so anyone can share it.
I’ve created a blogging site to not only share the events that caused my multiple attempts, but to advise on the warning signs. Follow lifeofbran.com and read my blogs, it’s intense, but it’s my life.
Kia ora Bran, and anyone else reading this. Just for others, be aware that Bran’s blog is very honest and detailed, so be careful if that will be difficult for you to read.
Dear Graham et al, so much of this is true, and yet there are other factors at work (as always). Many people take anti-depressants (starting with the issues above probably, not allowed to feel bad therefore take a pill) which have been strongly linked to suicidal ideation…. as well as other violence problems. Another issue society needs to consider in its risk: benefit ratio is that vaccine-induced brain injury, both subtle and not so subtle, causes symptoms of anxiety, depression, anorexia and other neurological disorders that look like psych issues (but are in fact medical issues, mostly chronic brain inflammation, auto-immune disorders and severe gut “the second brain” problems). The Innuit tribes said that they had never had “teen suicide rate” until the government started a vaccination program on their people. Trace mineral supplementation has been linked with a much improved mode, as well as sugar and junk food (too much glutamate, depletion of nutrients?) linked with poor mood. Farmers exposed to pesticides, herbicides, etc are noted to be suffering high levels of depression as well. What’s going on there? We need to start comparing data between groups to see if there are major underlying epidemiological issues that need dealing with, so we can start supporting people in a much more meaningful, holistic and helpful way. What ever we are doing right now, is not working terribly well. As a Social Credit candidate, I can’t help but agree that a chronic lack of funds is not good for individual, family, community, society and we have the policies to completely turn around financial insufficiency. kia ora, Tracy
Kia ora Tracy,
You and I can certainly agree that whatever we are doing now is not working particularly well. I also agree that public health work, including epidemiological studies are needed into the impact on our communities of the use of many substances in the environment that were investigated as individual products but rarely in their combined interaction with us in our real environment.
I am not convinced that the evidence is strong that there is a chemical component from vaccinations to suicide rates, whereas there is good evidence in many societies quite similar to ours that poverty, inequality and community structures collapsing are contributing factors. For example my own experience of depression is quite closely tied to the latter combined with my own individual lifestyle factors.
Anti-depressants are challenging and not all of my friends who have used them have found them helpful. However, I think it is important to say for those that might read this, that there is strong evidence that for many people anti-depressants or anti-anxiety medication may need to be part of the overall care plan to overcome depression, anxiety or psychosis. They are worth trying, but they can be hard work and it’s at least six weeks before you can draw a conclusion as to whether they help. In addition, it is often the case that people have to try different drugs and often varied combinations to find one that works for them.
I understand your concerns, Tracy, and indeed I support the right to choose to not use medication and avoid vaccinations. Finally, I know you’ll have a lot to say in response, but please remember that I don’t allow a continuous thread in my comments on my blog, and this initial comment is almost a blog in its own right. So please write it up into a blog in its own right rather than devote all your time to this comments section.
Heoi, Graham
P.S. I edited one story out of your comment because it could be quite triggering for people.